As an informatics nurse, it is important to create environments where nurses can work efficiently. One of the biggest challenges faced by nurses is they are inundated with information. Inconsistent documentation practices can also add to this problem. The way a chart is organized and the questions that prompt documentation should guide nurses through the charting process – not make it more difficult.
The patient record is an important communication tool for nurses and health care staff. It also serves as the legal record of care delivered to a patient. Taking the time to design and develop an effective charting format provides the foundation for nurses to enter and retrieve
Considering the following concepts can help organize nursing data in the patient chart. When a chart is well structured, the nurse can quickly find important patient information and act accordingly. Additionally, an intuitive system that allows the nurse to flow through the charting process can ensure that critical information is in the hands of those who need it at the right time.
1. Question Your Questions
Forms, documents, and nursing charts are designed to elicit information. However, how each question is phrased can make a difference in the data you are looking to collect. Ensuring each question is worded well can enhance the usability of the chart.
When questions are thoughtfully planned, it can help the nurse read and write in the documentation efficiently. It also improves the quality of the information by decreasing ambiguity and streamlining the nursing charting process.
When developing questions for a nursing chart, try answering a few of the following:
- Is the objective of the question clear?
- What part of the nursing process does the question seek to support?
- Can the question be shortened?
- Is the question actually 2 questions disguised as 1?
- Is the question too wordy?
Brevity is important but the primary objective
Question writing is a skill that can get better with time and practice. Continually reviewing and improving chart questions can assist in improving the quality of the nursing data you are looking to collect.
2. Know Your Point of View
Are questions asked from the point of view of the nurse or patient? Depending on the objective, either can be effective. The key is to be consistent with one point of view throughout each section of the chart.
A question that reads “was informed consent obtained?” is from the view of the nurse because it is the nurse performing the action. However, the question “do you have a family history of cancer?” is from the view of the patient because the question is directly aimed
When questions flip between different points of view randomly, it is jarring to the reader. If a shift in perspective does need to occur, create a new section to demonstrate that a new style of questions may follow.
3. Select Appropriate Answer-Types
Next, pay attention to what kind of answer you are looking to receive from your question. Most electronic health records offer a variety of answer-types like radio buttons, checkboxes, drop-down lists, etc. Ensure that each answer-type is appropriate to the question being asked.
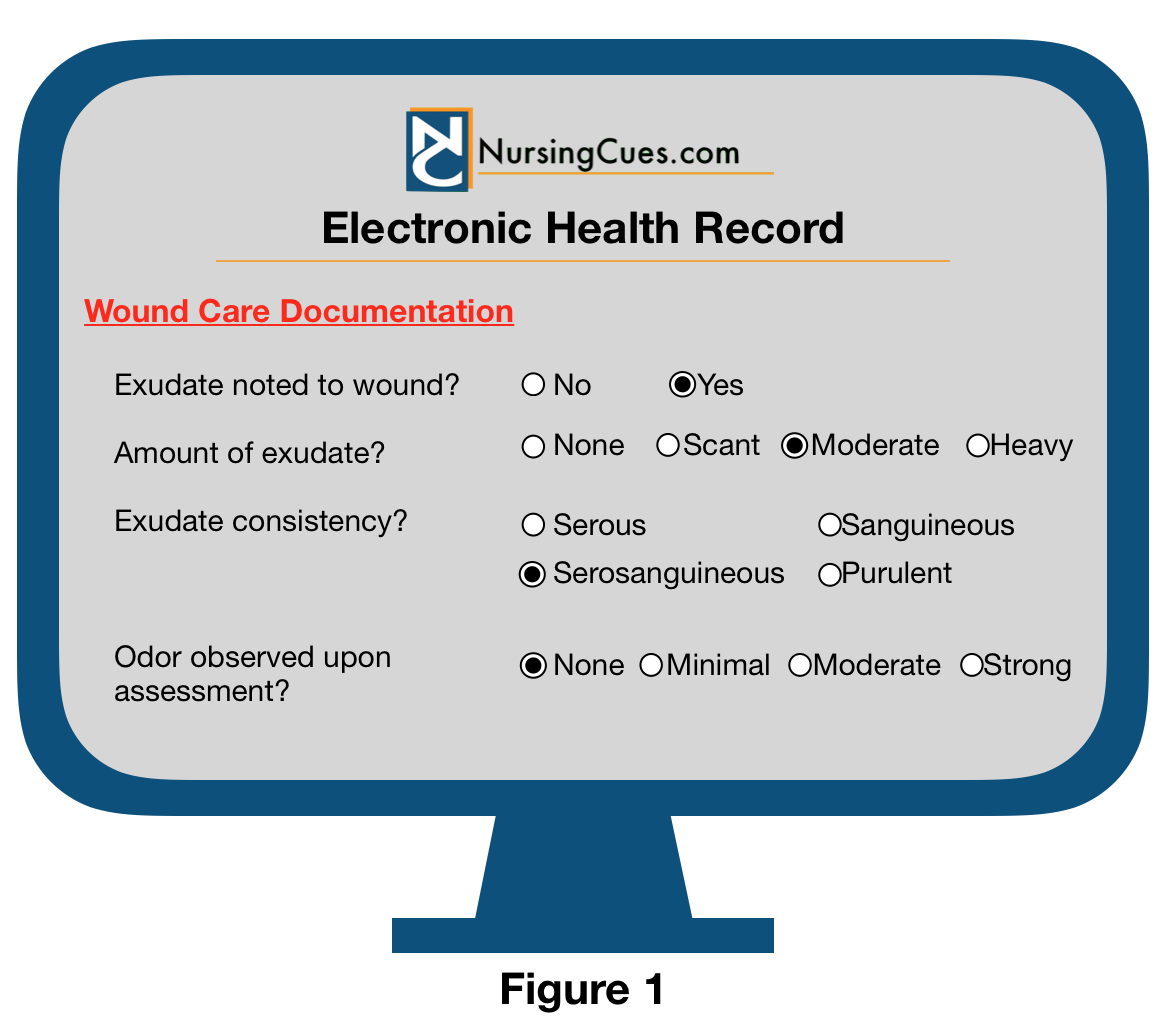
Take the time to learn the types of answers your electronic health record uses in response to questions. For example, a radio button forces the nurse to select only one answer among supplied choices. This type of answer format is appropriate for questions that have only one possible answer (see Figure 1).
 Some electronic health records have drop-down lists that allow the user to select multiple answers like when you see a Check All That Apply type question. If a chart uses a Check All That Apply answer-type for a question that should have only one possible answer, it can open the door to documentation errors. This is because more than one conflicting answer could be selected in addition to the intended response. Consider using these built-in functionalities with your question answer-types to prevent possible documentation issues.
Some electronic health records have drop-down lists that allow the user to select multiple answers like when you see a Check All That Apply type question. If a chart uses a Check All That Apply answer-type for a question that should have only one possible answer, it can open the door to documentation errors. This is because more than one conflicting answer could be selected in addition to the intended response. Consider using these built-in functionalities with your question answer-types to prevent possible documentation issues.
Another popular answer-type used in electronic charting is the checkmark. One would assume that a checkmark that appears on the computer screen would also display as a checkbox when the chart is printed. However, this is not always the case. In certain software systems, a checkmark answer-type signifies the answer
Figure 2 is an electronic health record where the nurse completed an unremarkable assessment. This electronic health record example translates a checkmark as a YES and a blank box as a NO. When the same assessment is printed or exported from the nursing chart, the document takes on a slightly different appearance (see Figure 3).

The basic idea that an unremarkable exam has been preserved. However, the word “Check” in the header Check if Within Normal Limits doesn’t make sense in the printed chart. As a result, a different answer-type format should be considered.
Evaluating the printed or exported version of the patient chart can help identify these variations. This will give you the opportunity to develop solutions and address potential issues.
4. Use Standardized Languages When Possible
Standardized languages are words and terminologies that have a standard code associated with a single term or concept that is accepted throughout the industry. These codes are often recognized nationally or internationally. Using a standard language allows information from one electronic health record system to send or receive information to another electronic health record system when the technical infrastructure is in place.
Using standardized nursing languages in a nursing chart makes it easier to maintain the database of the documentation system. This is because each term is assigned a unique code that is uniformly used by other health care organizations. Employing accepted standardized languages in the electronic health record makes it possible to pull data and create meaningful reports.
Examples of Standardized Languages include:
- NANDA International, Inc. – Nursing Diagnosis
- ICD-10- Medical Diagnoses
- CPT– Medical Services/Procedures
- RxNorm– Pharmacy
- SNOMED CT– Standard Clinical Phrases
- LOINC- Laboratories
Bonus Tip
If your electronic health record cannot display questions with
Final Thoughts
Effective management of nursing data in patient charts can facilitate the work of nurses on multiple levels. Taking the time to effectively review the question structure and answer-type format may enhance documentation practices. When intuitive charts that use standardized languages are created, data accuracy and reporting capabilities can be enhanced.
Good luck as you continue to improve your nursing documentation systems.

{kind=link}